
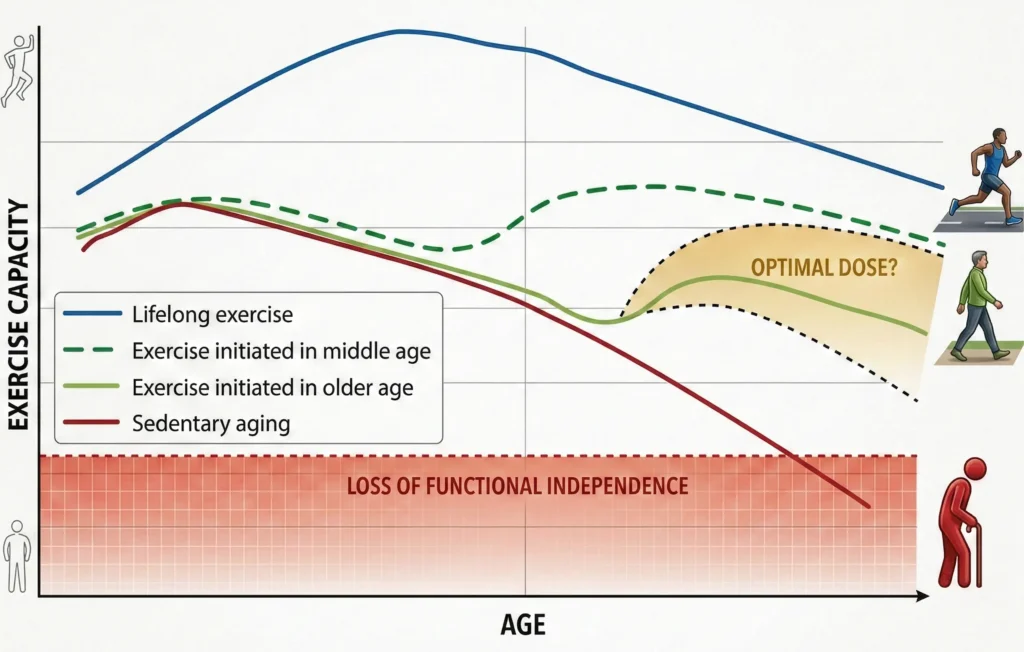
Most people view middle age (45–64) as a slow “fading out.” We focus on our careers and families while quietly accepting “creaks and aches” as an inevitable part of getting older. But science tells a different story: midlife isn’t the beginning of the end; it is your ultimate window of physical opportunity. It is the moment you decide whether you will merely “age” or whether you will thrive for the next forty years.
In this Muscle & Motion blog, we’ll explore how to bridge the gap between young adulthood and lifelong vitality through evidence-based training.
The silent threats: What’s really happening?
Midlife is associated with a gradual decline in muscle strength, power, and bone density and structural integrity. These changes directly impair force production, movement speed, and tolerance to mechanical stress. In the following sections, we will break down these physiological shifts to understand how they impact your body and, more importantly, how you can counteract them.
Muscle mass and strength reduction:
Aging brings a natural, gradual decline in muscle tissue, but from midlife onward, this process specifically targets your Type II (fast-twitch) fibers. These fibers are responsible for producing force rapidly and generating power, the capacity to exert force quickly and effectively. As their proportion decreases, the muscle becomes less capable of responding to everyday functional demands, particularly tasks that require speed and force, such as rising from a chair, climbing stairs, or recovering from a loss of balance. Consequently, therate of force development and overall power decline are manifestations of muscle mass decline. When strength and power fall below the threshold required for routine activities, functional performance deteriorates. Over time, this combined structural and functional decline may progress to sarcopenia, a clinically recognized condition associated with increased risk of disability.
To learn more about the different types of strength and the differences between them, read our blog: Understanding Strength: A Deep Dive into Its Types and Foundations.
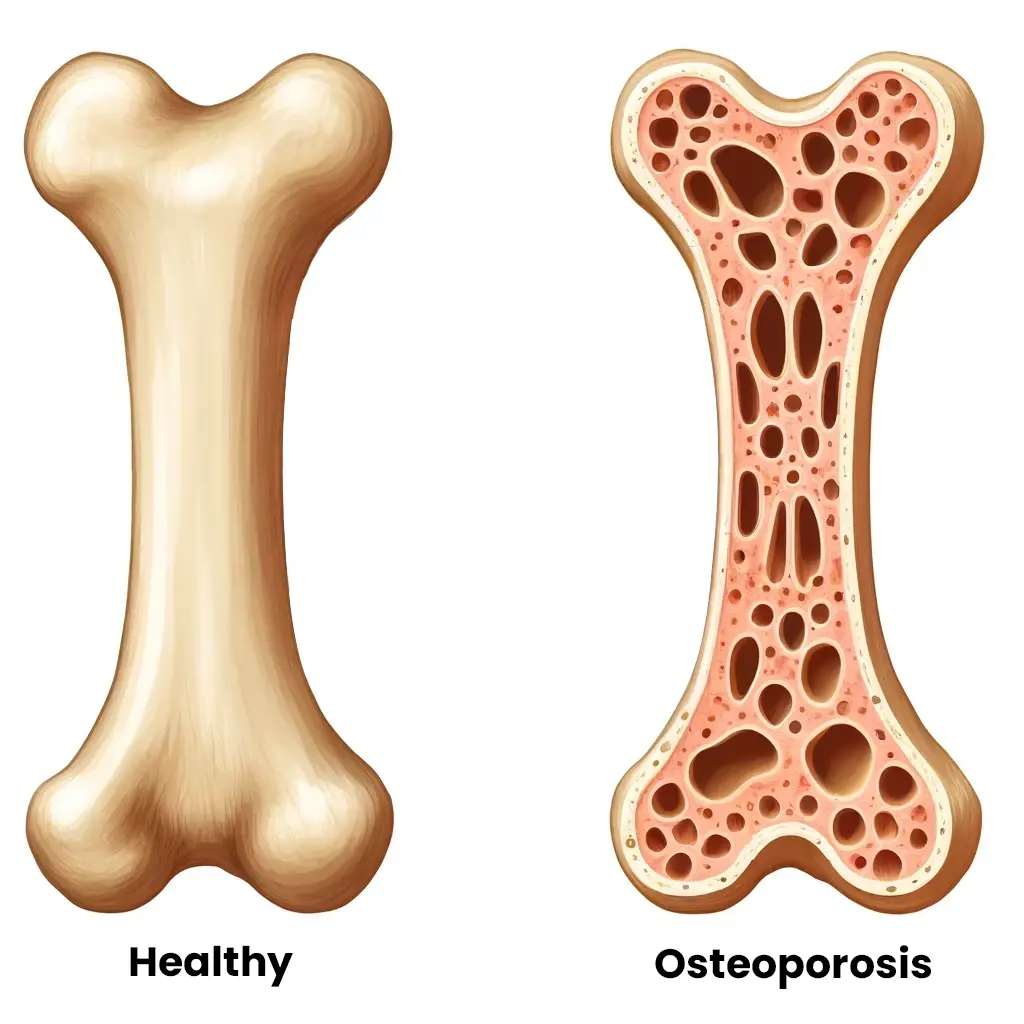
Bone density and structural decline:
With aging, bone mineral density (BMD) declines, and the internal supportive structure of bone becomes thinner and less connected, while cortical bone undergoes thinning and increased porosity. These changes reduce overall bone strength and load-bearing capacity. In women, this process accelerates markedly after menopause due to the decline in estrogen, placing postmenopausal women at substantially higher risk of rapid bone loss and fragility fractures. When bone loss reaches clinically significant levels, it is defined as osteoporosis, a condition characterized by low BMD and increased susceptibility to fractures following minimal trauma. In the presence of reduced muscle strength and power, the likelihood of falls and fracture-related injury increases further.
To learn more about protecting your skeletal health, read our blog: Enhancing Bone Density Through Exercise
Rise of chronic conditions:
Midlife is associated with a marked increase in the prevalence of chronic conditions, including obesity, type 2 diabetes, cardiovascular disease, and osteoarthritis. Epidemiological data indicate that approximately 18–36% of middle-aged adults live with at least one chronic disease, while up to one-third experience multimorbidity, the coexistence of two or more conditions. These chronic health issues, particularly arthritis and musculoskeletal pain, act as major catalysts for accelerated functional decline, heavily contributing to early mobility limitations and physical disability
The culmination of these musculoskeletal, neuromuscular, and metabolic factors directly impacts the ability to perform activities of daily living. Because of decreased strength, stiffening joints, and impaired balance, the estimated annual prevalence of falls triples from 9% in adults aged 40 to 44 to 28% in those aged 60 to 64.
Resistance training as a primary countermeasure
Muscle disuse is a modifiable contributor to age-related decline. Resistance training is an effective non-pharmacological strategy to counteract sarcopenia, preserve bone mineral density, and improve metabolic health. Importantly, midlife remains a highly responsive period for muscular adaptation. Studies show that both men and women can achieve significant hypertrophy, including increases in Type II (fast-twitch) fiber size, following progressive resistance training. Even moderate-intensity training (~60% 1RM) over 24 weeks has been shown to increase thigh muscle cross-sectional area by up to 7% and substantially improve strength.
For general strength and hypertrophy, guidelines recommend training two to three times per week, performing two to three sets of multi-joint exercises per major muscle group at 70–85% of one-repetition maximum (1RM).
The missing link: Why you need power
Studies indicate that skeletal muscle power declines faster than maximal strength with aging. Therefore, midlife training programs should intentionally target power development alongside maximal strength and endurance.
How to train for power:
Power development requires high-velocity resistance training, performed by executing the concentric (lifting) phase as rapidly as possible while maintaining a controlled eccentric (lowering) phase. Effective training loads are typically moderate, around 40–60% of one-repetition maximum (1RM).
Power can also be developed through explosive-strength exercises and plyometric training, which incorporate rapid stretch-shortening cycle movements such as jumps, hops, and medicine ball throws. These methods enhance neuromuscular activation, rate of force development, and the capacity to generate force quickly under functional conditions.
Balance and functional capacity
Optimal midlife training should integrate strength and power development with dynamic balance training. Functional training emphasizes multi-joint, task-oriented movements that reflect the physical demands of daily activities. Programs that challenge control of the center of mass, incorporate closed-chain weight-bearing exercises, and progressively narrow the base of support improve both static and dynamic balance. These adaptations enhance postural control, reduce fall risk, and support long-term functional independence.
Train functional movement
Midlife training should focus on “compound” movements – patterns that use multiple muscle groups at once to build strength, power, and balance simultaneously. You don’t need hours in the gym to see results. Even a “minimal effective dose” can create meaningful changes, provided you train with sufficient intensity. When time is short, prioritize these multi-joint, weight-bearing exercises to maintain your muscle mass and independence without needing excessive volume.
1. Squat variations
Why: Squatting strength is strongly associated with lower-limb power and functional independence. It directly supports the ability to rise from a chair, toilet, or low surface, a fundamental requirement for daily living.
2. Deadlifts
Why: Deadlifts strengthen the posterior chain and develop the capacity to safely lift objects from the floor.
3. Pressing and rowing movements
Why: Multi-joint upper-body exercises maintain pushing and pulling strength, preserve lean mass, and support everyday tasks such as pushing doors, placing objects overhead, lifting items onto shelves, or pulling objects toward the body.
4. Single-Leg Training
Why: Improves unilateral strength, corrects asymmetries, and challenges dynamic balance, all critical for fall prevention, gait stability, and tasks such as climbing stairs.
5. Calf raises
Why: Maintaining calf strength directly supports mobility and fall resilience.
6. Farmer’s carries
Why: Improve grip strength, trunk stability, and real-world load-carrying capacity (e.g., carrying groceries or household objects).
7. Jump and power exercises
Why: Train rapid force production, improve rate of force development, and preserve neuromuscular responsiveness.
In summary, midlife is not the beginning of the end; it is a critical window of opportunity. By shifting your focus toward resistance training, prioritizing muscle power, and challenging your balance, you are doing more than just staying active – you are actively rewriting your biological age. Investing in these foundational movements today ensures that you don’t just live longer, but that you remain strong, capable, and independent for decades to come.
At Muscle and Motion, we believe that knowledge is power, and understanding the ‘why’ behind any exercise is essential for your long-term success.
Let the Strength Training App help you achieve your goals! Sign up for free.
References:
- Hayek, R., Gutman, I., Baranes, G., Nudelman, Y., & Springer, S. (2024). Smartphone-Based Sit-to-Stand Analysis for Mobility Assessment in Middle Age. Innovation in aging, 8(10), igae079. https://doi.org/10.1093/geroni/igae079
- Peeters, G., van Schoor, N. M., Cooper, R., Tooth, L., & Kenny, R. A. (2018). Should prevention of falls start earlier? Co-ordinated analyses of harmonised data on falls in middle-aged adults across four population-based cohort studies. PloS one, 13(8), e0201989. https://doi.org/10.1371/journal.pone.0201989
- Cruz-Jentoft, A. J., & Sayer, A. A. (2019). Sarcopenia. Lancet (London, England), 393(10191), 2636–2646. https://doi.org/10.1016/S0140-6736(19)31138-9
- Morin, S. N., Leslie, W. D., & Schousboe, J. T. (2025). Osteoporosis: A Review. JAMA, 334(10), 894–907. https://doi.org/10.1001/jama.2025.6003
- Hurst, C., Robinson, S. M., Witham, M. D., Dodds, R. M., Granic, A., Buckland, C., De Biase, S., Finnegan, S., Rochester, L., Skelton, D. A., & Sayer, A. A. (2022). Resistance exercise as a treatment for sarcopenia: prescription and delivery. Age and ageing, 51(2), afac003. https://doi.org/10.1093/ageing/afac003
- Peterson, M. D., & Gordon, P. M. (2011). Resistance exercise for the aging adult: clinical implications and prescription guidelines. The American journal of medicine, 124(3), 194–198. https://doi.org/10.1016/j.amjmed.2010.08.020






